A quick note at the beginning. This article is really only relevant for cis men. I will be publishing content in the future which is more suitable for women, enbees, trans people, etc; in short you probably want to avoid androgenic hormones and focus on other performance enhancers such as peptides, SARMS, and weird-arse agonists of non-androgenic hormones.
I’ve been conducting what I cynically refer to as “phase one trials” with various performance enhancing compounds. Like the more organised and curated pharmaceutical namesake, the aim of my experiments have not been too fully understand the nature and effect of each compound – that takes time. It’s been more about ascertaining the approximate dose I may want to run in the future, noting tolerability (any obvious side effects for instance), and a getting rough “feel” for each drug. Let’s say it’s been about taking a shortlist of candidate compounds and making it shorter, and as I revisit each of them I’ll record my experiences here.
Many, if not all of the drugs I’ve been experimenting with have the effect of suppressing natural testosterone production. This is one of two reasons why I’ve been administering a weekly “base” of testosterone undecanoate throughout the whole venture. I’ll elaborate in a future post on the necessity of using testosterone while running synthetic anabolic steroids, but meanwhile let’s talk about the other reason as its a bit more considered and a bit more applicable to athletes.
When I decided to begin this journey the first thing I did was to test my natural levels of a bunch of hormones, liver enzymes, cholesterol biomarkers, and anything else that can potentially be effected by anabolic steroids. I’ve always found it pretty easy, if not too easy to put on muscle mass, so I was a little surprised when I found out that my testosterone levels were on the low side of normal.

This is what’s probably been happening: when you’re reliant on natural testosterone production your testicles (assuming you own testicles) squirt small amounts of the hormone into the blood stream throughout the day. Levels are highest in the morning and lowest in the late afternoon. The daily volume of hormone produced is reliant on many factors: BMI, age, diet, sleep, stress levels, and most importantly in my case how hard you’ve been training.
To a point, exercise increases natural testosterone levels but hard training sessions deplete natural production, leading to a kind of bell curve. Climbing five times a week at the age of 49 is almost as counterproductive to maintaining natural testosterone levels as sitting on the sofa watching daytime tv and eating pizza for breakfast. If you’re interested in maximising natural production a moderate load of exercise with frequent rest days is the way to go. This is something that Lattice Training (for instance), spend a lot of their time trying to convince their customers: less is more. Bit it’s something I want to push beyond.
So what’s so special about testosterone anyway? In the male body, as the primary anabolic hormone its responsible for promoting protein accretion in the muscle tissue, and this results in increased rates of recovery from exercise. As such, crashing your testosterone levels by over-training leads to reduced recovery rates and that’s an issue that can be hacked by supplementation with an exogenous source of hormone.

One important aspect to understand is that supplementing exogenous testosterone has the effect of shutting down your natural production. Your Hypothalamic–pituitary–gonadal axis (if you’re a cis male), senses that there’s enough testosterone floating around and doesn’t bother making more. So if administered intelligently (we’ll get into the details of that in a minute), you’ll replace the diurnal, pulsatile production of endogenous testosterone with a steady, constant source which remains optimal regardless of how often you train, if you’ve managed to have enough sleep, or if you couldn’t resist eating all 5 of those donuts in one sitting.
So what about the dose? The obvious assumption to make when supplementing testosterone would be to push into supra-physiological levels, IE somewhere above the 32.63 nmol/L cutoff that the blood testing service I use considers the upper end of their natural reference range (see diagram at top of page). After all if a moderate dose helps increase work capacity a little, then a less moderate dose must help a lot, right? Actually in climbing as in many other sports where power to weight ratio is a consideration, this isn’t actually the case.
In the a study titled “Testosterone dose-response relationships in healthy young men”, the researchers gave varying amounts of testosterone to men and measured their resulting weight gain. Higher doses led to more weight gain so if you’re trying to stay light then you want just enough testosterone to replace your natural level. That way, morning or evening, whatever your allostatic load, you’ll recover at a rate that’s optimal for you. Or if you already have a problem with recovering optimally, you can dial in your testosterone levels to near the top of the “normal” range to optimise recovery, and if you start putting on weight drop the dose until you reach a happy balance. This obvious requires regular testing, which you should be doing anyway if you’re taking exogenous hormones.
There are various esters of testosterone available. Different esters have different serum half lives. For instance if you inject testosterone propionate today, in 4.5 days time you’ll have half of it left in your system. If you inject testosterone cypionate, it will take around 8 days.
If you’re a competitive athlete concerned about the possibility of drug testing, a shorter acting ester may be more appropriate because it can be out of your system with minimal planning. A bodybuilder who goes on and off cycle might use a medium acting ester; that way when they’re finished with the cycle they don’t have to wait months for the drug to clear out of their system. But for me, as someone who’s planning to dial in the right dose and stay on it, it makes sense to use a long-acting ester as this will lead to the most stable levels. Seeing as what’s most important to me is unvarying levels, morning and evening, whatever I’m doing, the longer the half life the better.
The longest acting ester I have access to is testosterone undecanoate so that’s what I use. With a half life of around 21 days it takes quite some time for serum levels to stabilise so it’s a long-term endeavour to test, tweak, test, etc. The plus side however is that it’s leads to extremely stable and unvarying hormone levels which is the point of the whole exercise.
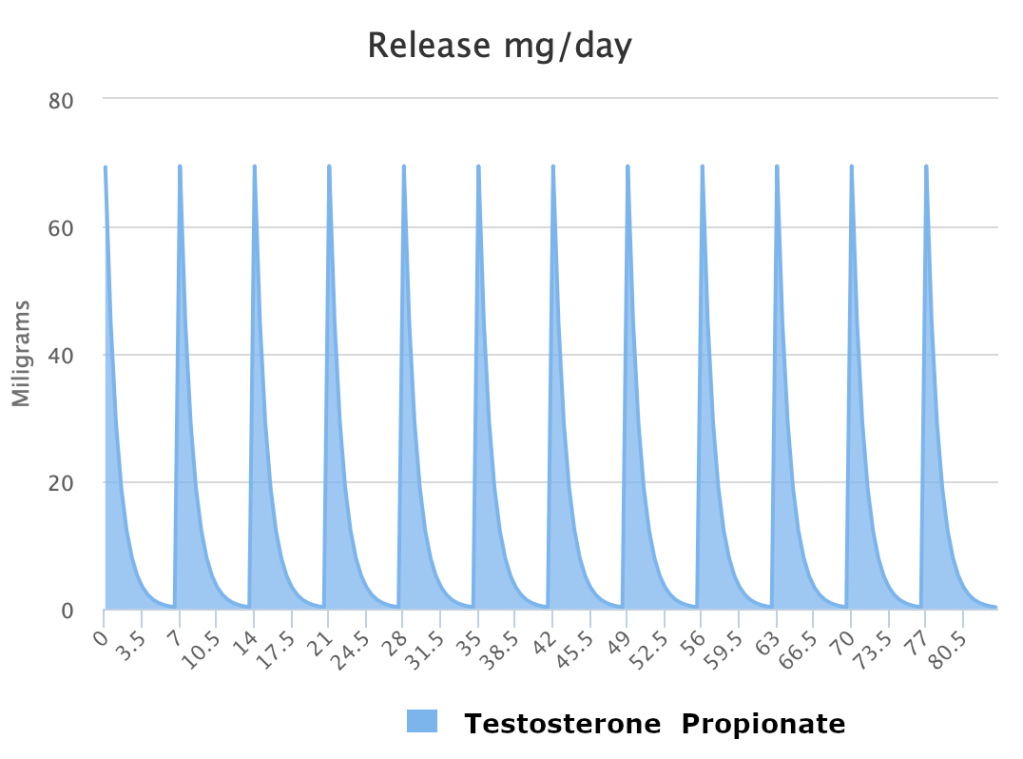
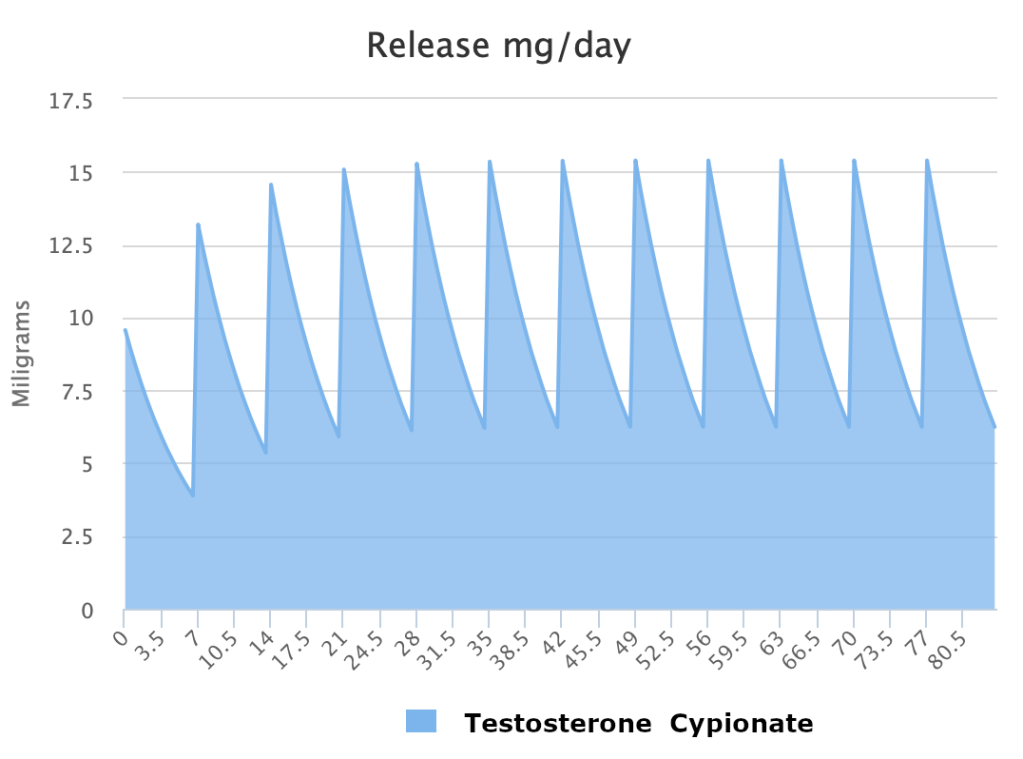
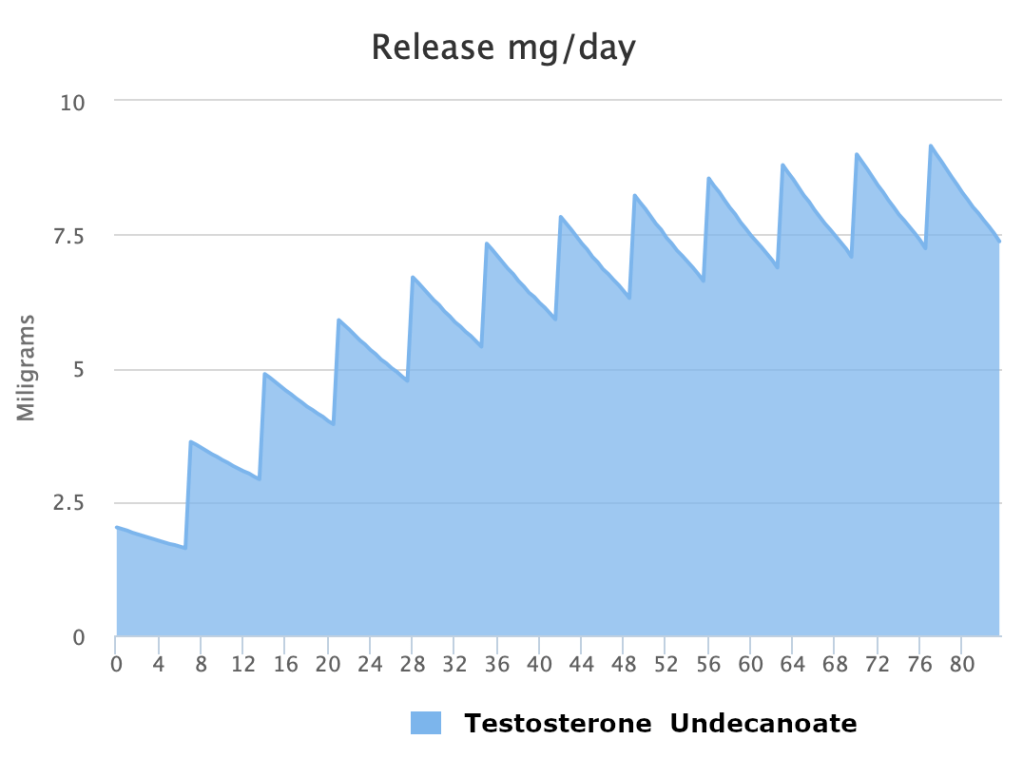
Above are three screenshots from steroidplotter.com comparing blood serum concentrations of three different testosterone esters administered at 100mg once per week. As you can see the short-acting ester (testosterone propionate) takes no time to reach maximum blood serum concentration but by the end of the week there’s nothing left in the system. The long-acting ester (testosterone undecanoate) takes the full 12 weeks to reach stable blood serum concentration but is the most stable of the three showing similar levels at the beginning and end of each week. The medium acting ester (testosterone cypionate) is a compromise between the two extremes.
Regarding administration frequency, I was going to go into detail about the considerations around this but the post is already pretty long and detailed. I’m going to split the subject into a separate post and put it up when I’ve had more time to thoroughly research how changing administration frequency can be used to manipulate SHBG levels.
Many users administer testosterone undecanoate once every 8-12 weeks and although this is possible it leads to the same yo-yoing of hormone levels you’d get from more frequent administration of a shorter acting ester. Conversely I don’t love needles so injecting every day wouldn’t be preferable, in fact it would be a massive pain (quite literally) in the arse. Once a week seems to me to be a good compromise between convenience and stability, and leaves room to tweak up or down if necessary.
In summary, exogenous administration of testosterone, particularly frequent administrations of a long acting testosterone ester like undecanoate as a means of keeping testosterne at a pre-planned level at all times of the day, no matter what else is going on has significant effects on ability to recover. Which means you can train harder, wake up the next day with optimal levels, and do it again.
On a final note, it occurred to me while I was writing this post that it’s actually possible to use testosterone for the purpose of reducing hormone levels if needed. Why would you want to though? Say your natural levels were abnormally high and you had a problem with putting on muscle weight when you didn’t want to. Well, taking exogenous testosterone shuts down your natural production, so you could dial it in at a lower level than that which your tesicles would have produced and avoid the problem. Very hypothetical I know but fun to think about.
