This is going to be more of a pondering than a report into self experimentation. So far I’ve taken a few small doses of Nandrolone Decanoate to judge its tolerability, and I’m about to start adding 50mg to my weekly testosterone injections. This is a quick explanation as to why I might want to do this.
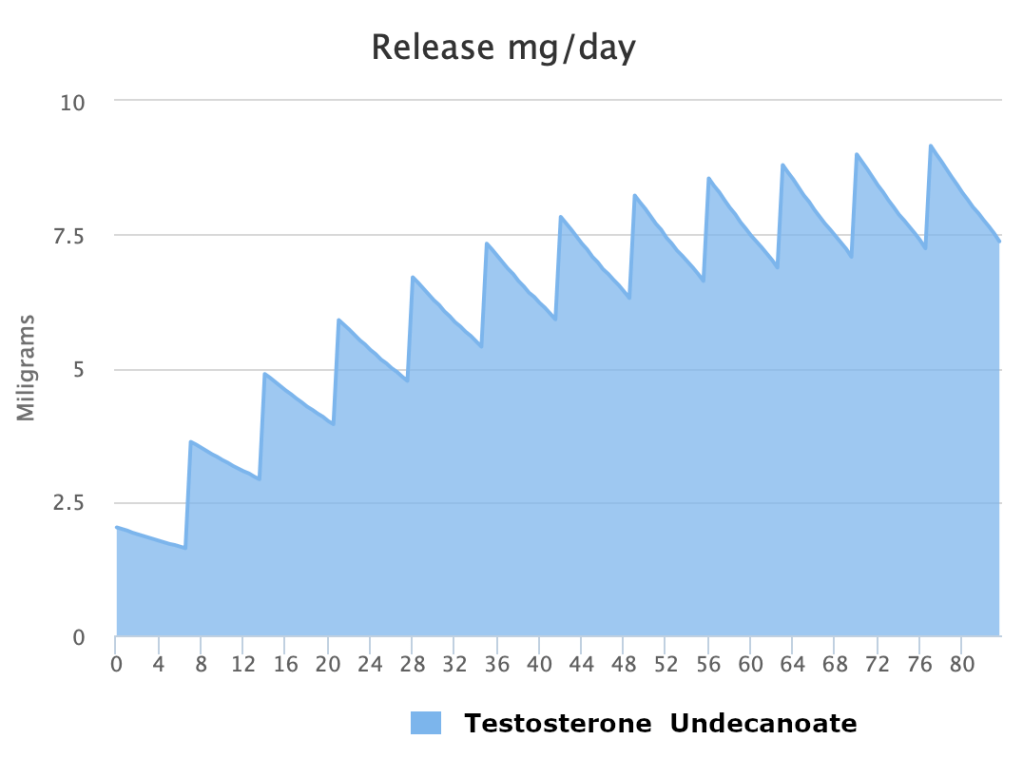
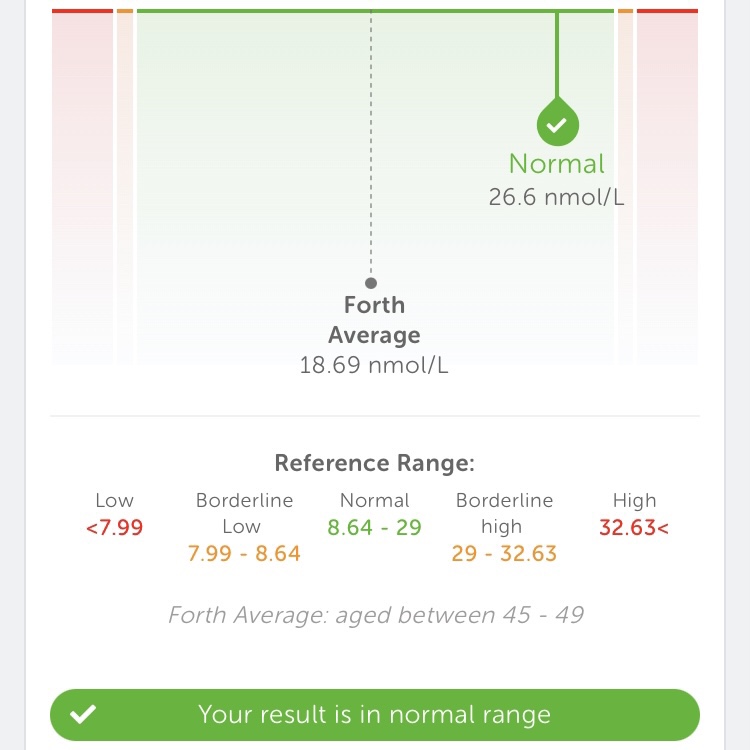
After about 7 weeks of taking Testosterone Undecanoate at 250mg a week, I took a blood test as a quick interim check to see what my levels were. I didn’t do a full blood panel, I just checked total testosterone so I can adjust up or down accordingly before re-testing estrogen levels and all the other stuff that I’ll need to keep in range over the long-term. As you can see from the image below, my levels had doubled since the last blood test but were still a little lower than I was expecting from the dose. Ideally I’d want it to be into the “borderline high” area of the reference range: IE optimised without being supra-physiological.
This unexpectedly low value could be caused by one or more of the following factors:
- It could be that with such a long ester of testosterone, my levels hadn’t fully had a chance to stabilise. 7 weeks wouldn’t usually be long enough to achieve stable blood serum levels from such a long-acting ester but I had “front loaded” in the first few weeks and calculated that I’d have reached saturation by this point. However it’s possible that regardless of my diligence that dose by dose, week by week, the drug was still accumulating in my system
- The “underground lab” I was using to supply the testosterone may have under-dosed the product leading to me taking a smaller dosage than I had intended
- There’s some evidence to show that intramuscular injections into the medial deltoid might provide suboptimal bioavailability compared to administration into the ventrogluteal muscle. As I was rotating between these two muscle groups, half my shots might have had a less potent effect than the other half
- The dose might have just been too low. There’s considerable variation from person to person regarding the relationship between dose administered and resulting blood serum levels. Maybe I excrete the drug faster than the average person or maybe my body cleaves the ester off the parent molecule less efficiently.
I decided to take the following actions and test again in 15 weeks:
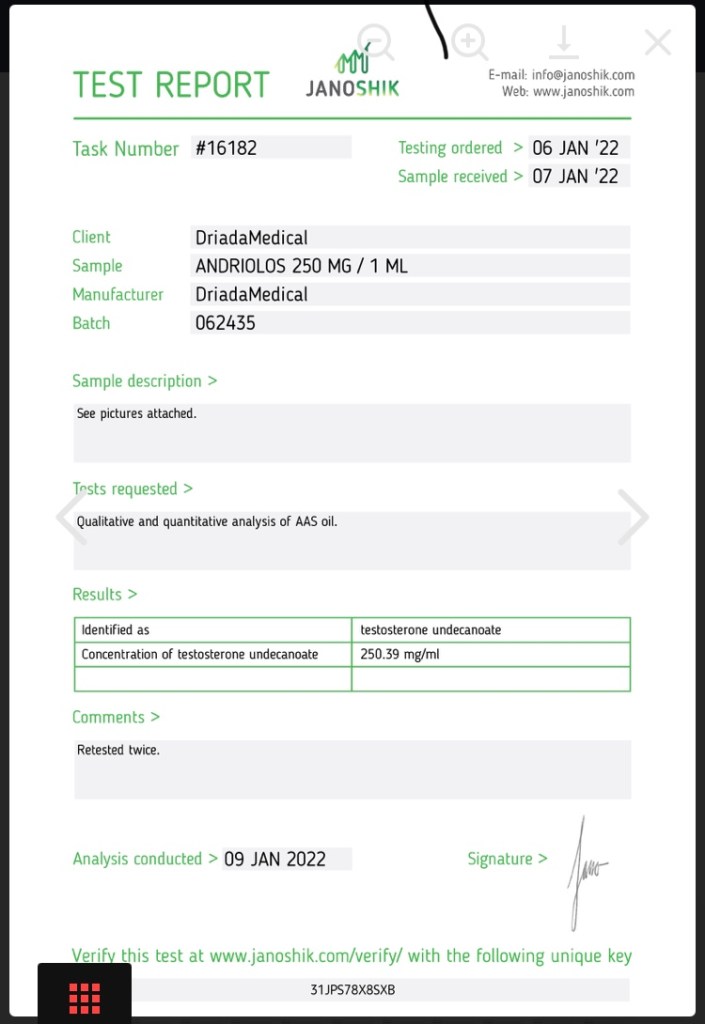
- I switched to a supplier who provides traceable batch numbers and publishes lab test results for each batch
- I’m standardising my injection site protocol: one week in the left ventrogluteal, one week in the right ventrogluteal, and repeat
- I’m upping the dose from 250mg to 300mg per week
Anyone who’s familiar with scientific standards will have immediately spotted a red flag; the first rule of experimentation is to change one variable at a time. However two of the three changes I’m making to my protocol are more about standardisation than optimisation so will provide a good base to gain maximum insight into the next round of blood test results.
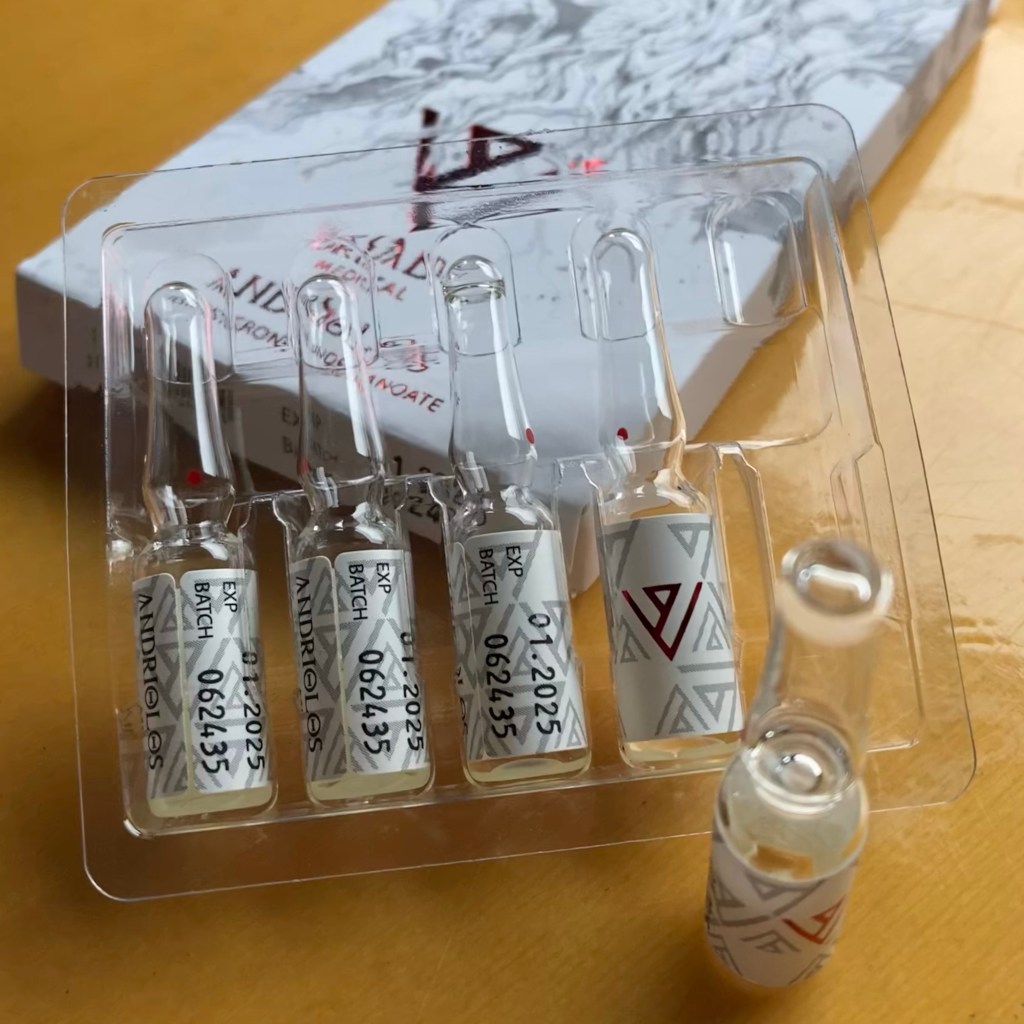
My new supply of testosterone is provided in handy 1ml, single use ampoules, each containing 250mg of testosterone undecanoate (providing 157.9mg of testosterone once the ester has been cleaved off by biological processes). The issue is that unlike drawing a dose of one’s choosing from a 10ml vial (how my previous supply of testosterone was packaged), I’m now stuck with dosing in multiples of 250mg.
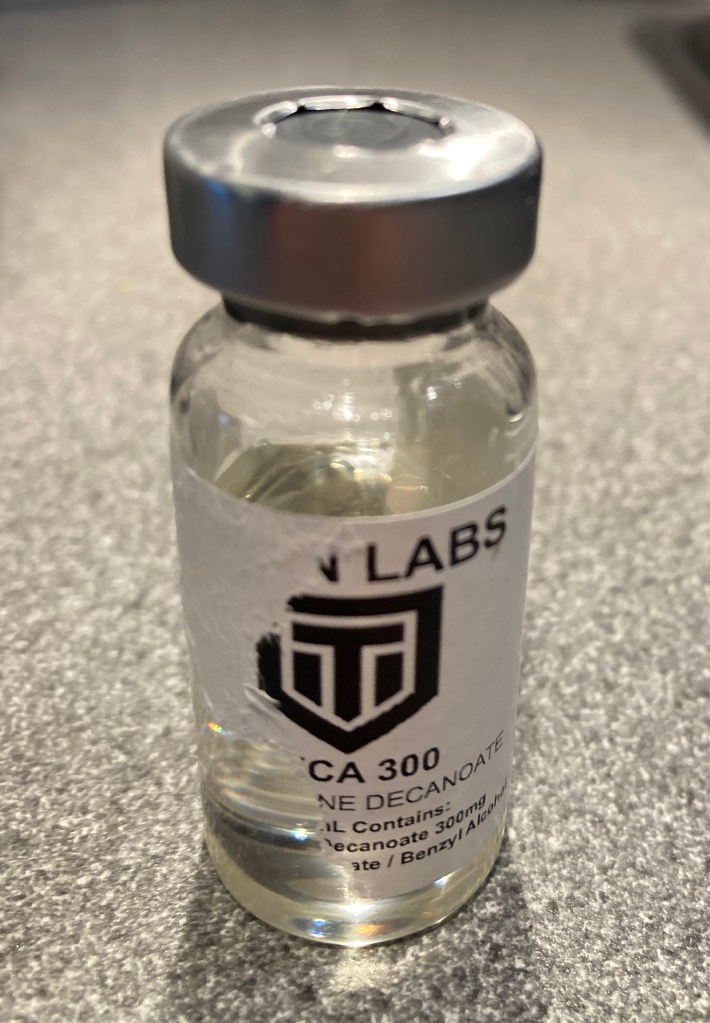
One easy strategy to circumvent the ampoule size issue is to keep the dose the same and change the administration frequency instead. So if I want to increase my levels I can inject every 6 days instead of every 7. Conversely if I want to reduce my levels I can inject every 8 days. But there’s actually something else I can do which kills two birds with one stone in a particularly elegant way: I can top up the weekly dose with 50mg of Nadrolone Decanoate.
So why might I want to do this? Anecdotal reports from generations of athletes who dope with Nadrolone have made a pretty clear case that it has a significant effect on reducing joint pain. This has been backed up by clinical trials and the results are very convincing. As a 49 year old climber, my fingers are continually achey, creaky, and a bit crackly. Nadrolone might be the perfect remedy and I get the benefits for free as a result of tweaking my year-round testosterone protocol.
It’s not entirely clear why nandrolone has such a demonstrable effect on joint pain but there are two commonly cited hypotheses (yes I had to look up the pleural of “hypothesis”):
- It may potentiate collagen synthesis leading to cartilage deposition in the joints
- It’s a rather “wet” compound so the effect might be the result of increased synovial fluid production.
It would be great if point one was the case because increased collagen synthesis would also aid in tendon health, and therefore reduce the likelihood of a training-induced finger injury. Point two would suck because fluid retention (as we’ve discussed so many times so far) is bad for climbers who care so, so much about strength to weight ratio. The likelihood is that both hypotheses (I looked it up a second time to double check that it actually is the pleural of “hypothesis”) are correct and contribute to the beneficial effects on joints.
So if I’m upping my dose by adding a second compound, how do I know if I’ve reached my desired hormone level when I do my next blood test? Conveniently the ECLIA test employed by the service I use actually can’t tell the difference between nandrolone and testosterone, so the serum level i get back from them will actually be a combined serum level of testosterone and nandrolone. Convenient eh?
At this point everything seems to be falling conveniently into place. The half life of Nadrolone Decanoate is long enough that the two drugs can be administered with the same frequency, and therefore together in the same injection. Also nandrolone is actually present in small concentrations in both the male and female natural endocrine environment, so my protocol can still be classed (if anyone cares), as bio-identical hormone replacement.
There are however potential downsides to using nandrolone year-round: there are plenty of anecdotal reports of the drug causing depression, anxiety and increasing incidents of jealous, possessive ideation, and this has be backed up by research. These mental effects are usually reported at much higher doses than I’m planning to run, but it’s certainly something I’m going to be diligently looking out for. There is research to show that nandrolone messes with dopamine transport proteins and monoamine oxidase function. I don’t want to be fiddling with my brain chemistry in that way. Also as I alluded to earlier, nandrolone is notorious for promoting fluid retention in a dose dependent manner. Both of these issues are a good reason to stay around 50mg which is a very low dose in comparison to that taken by most athletes. Which brings me conveniently on to…
How do I know that the 50mg dosage necessary to top up my weekly testosterone protocol is enough to lubricate my finger joints? In short, I don’t. The Tatem, Holland, Lipshultz paper I linked to above presents evidence that “Deca” (as nandrolone Decanoate is colloquially known) was efficacious at reducing joint pain at a median dose of approximately twice that which I’m planning on taking. I have three grams of the stuff so I might as well give it a go. It may require some future fiddling, or my plan might not be feasible at all. I’ll start at 50mg a week because it fits into my protocol and play around with things if I need to. I think it’s more probable though that if I don’t get what I’m looking for at 50mg, or I experience depression or water weight, I’ll chalk it up to an interesting experiment and revert to testosterone only.
A quick note: many if not all of the anabolic steroids discussed in this blog have the effect of suppressing or “shutting down” natural testosterone production, but nandrolone particularly so. I wouldn’t have chosen to use it unless I was committed to long term hormone replacement. Restarting ones testicular production can be a lengthy and difficult process.